A very perceptive nurse made this thought-provoking comment on my last post: “It has been a strange combination of arrogance and ignorance that has led us here.” She is dead on right…..But why and how have our healthcare leaders, at least on the medical side, developed this “strange combination”? We’ve worked on it, and we have worked very diligently perfecting this strange combination.
In my first post, I discussed how medical education has failed us. We neglected critical thinking, ethics, courage, integrity and moral reasoning in admission into our profession and in advancement in it. But why do we neglect this, when it has such an obvious negative result? Physicians, particularly academic physicians and those in leadership roles have been infected. Yes, infected. It is ironic that a viral pandemic could uncover a different, but perhaps equally deadly, kind of infection. This infection was never covered in medical school. It is unknown in microbiology, virology or parasitology. It is not taught in the prestigious schools of medicine. It is not covered at the Summer Institute of Tropical Medicine and Public health at Johns Hopkins or even the London School of Tropical Medicine. But it should be. We have been infected with a meme.
Let me try to explain with a personal story: In 2005 I was at the very pinnacle of my career as an Oculofacial Reconstructive Surgeon. I was a Full Professor at a midwestern medical school. I had published a number of papers and book chapters, given countless presentations at national and international meetings, won a number of awards for my research and served as the Secretary of Education for my subspecialty society. Then, one day thing changed. Years of not paying to ergonomics as I operated for hours with a heavy headlight on my head and flexed my neck, concentrating on surgery done under magnification, had taken their toll. I herniated a cervical disc and lost most of the sensation and fine motor skill in my dominant right hand.
I had spent years as a Chief Quality Officer (that can be a topic of another post). More times than I wish to remember, I had to take an older surgeon aside and gently suggest that he or she should consider retiring as they just couldn’t do the job as well as they should. I knew I was not up to my highest standards, and I didn’t want somebody to have to take me aside and tell me that. My patients deserved the best, and if I couldn’t do that any longer, it was time to move on. I may have retired from surgery a bit early, but much better than a bit late…
So I had to explore other options. I had more than a decade in Quality Improvement. I was a Black Belt in Six Sigma. I had led a large hospital in all of their programs and had some great successes. But I also had unexpected failures. I thought maybe an advanced degree could help me. I was already a member of what was then the American College of Physician Executives, and looked into their programs in Medical Management. I have to confess, I gave the highest rank to the program that was starting the soonest, which was at the Marshall School of Business at USC. It was a hybrid program, with 4 10-day in-person sessions and the rest online and independent. So I grabbed it.
Sometimes the best decisions are made by accident…or by Providence. This was one of those decisions. The program was absolutely amazing. I met some very impressive people—my classmates as well as teachers. Perhaps the most impressive was Dave Logan, whose mentor had been Warren Bennis. Dave introduced us to “Organizational Culture” as the primary determinant of Organizational Performance. He had spent a decade studying various organizations and companies and found that they fell into 5 Levels based on mood and language1:
Listening to Dave Logan in class and reading his book made me feel as though he somehow had a secret window on my own professional experiences.
Professionals usually cap out at Stage Three. Attorneys, accountants, physicians, brokers, salespeople, professors, and even the clergy are evaluated by what they know and do, and these measuring points are the hallmarks of Stage Three. “Teams” at this point mean a star and a supporting cast— surgeon and nurses, senior attorney and associates, minister and deacons, professor and TA’s.2
A typical faculty meeting shows the limitations of Stage Three. One professor after another gives his opinion and says what he thinks should be done. The result is that most educational programs look as if they had been designed by a committee—because they were. Students often ask if faculty ever speak to one another, and the answer is ‘not often’—at least about important topics.3
Understanding the culture of an organization is more than just academic in nature. It has an intimate relationship with productivity, both individual and collective. as There is a non-linear jump in what can be done with each step forward. This productivity jump is a key component in motivating leaders to assess their own culture and learn how to advance their own, and influence those around them.
Another key observation is that it is only possible to move one stage at a time. You can only become a Stage 4 organization by passing through Stage 3 first. Dave told a story about a consultant who was asked to aid a company mired in Stage 2 mood and language. The consultant had a vision of the future of what could be done at a Stage 4 level. Impassioned motivational talks and attempts at building teams were met with mostly a stony silence. Then one morning the consultant drove to the company and saw that his dedicated parking spot had been jackhammered free of the pavement, the area covered with sod and the parking sign removed. He was able to understand the subtle message.
The linear transition between levels works both ways. Organizational Culture is fluid, based upon internal and external pressures on the organization. Attaining a Level 4 culture is no guarantee that the organization will stay there! Dave Logan and I would go on to explore agent based modeling in an attempt to visualize the relationship between the elements of Organizational Culture and how it translates into Organizational Performance. We continued to hone our definition of Organizational Culture and ended up, at least for now, with this: The pattern of, and capacity for, adaptation based on a shared history, core values, purpose and future seen through a diversity of perspective. We realized that the mood and language as a means of shaping culture means that it is transferred as a meme. It has the ability to transform as well as imparts an ability and a pressure to share with others. It acts as an infection!
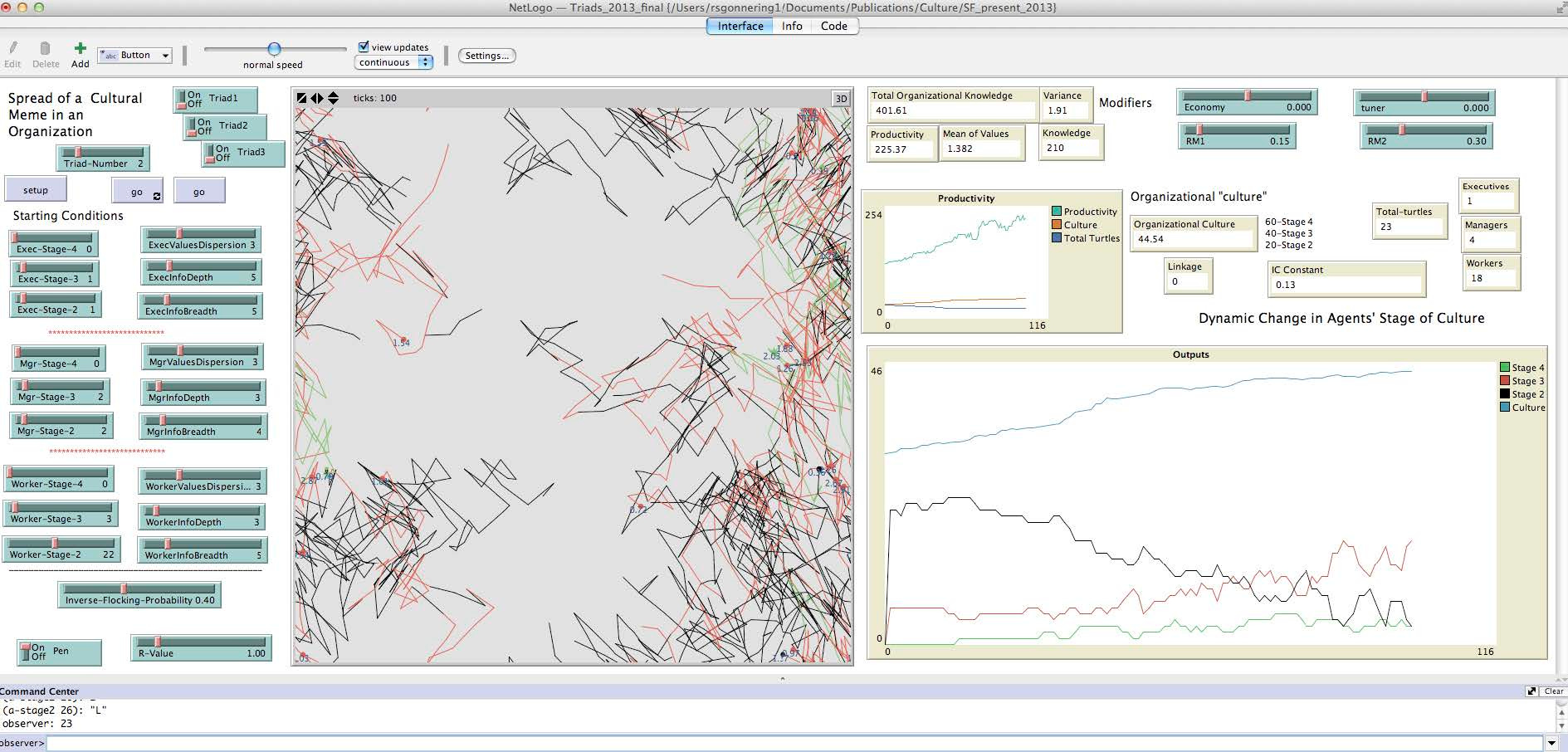
Within an organization, there will be members at various levels of internal culture. They will interact through synchronous contact as well as asynchronous communication, such as written or electronic. Our model first showed the ability to create an organization that would remain stable at a Level 3 culture in response to stochastic variation in internal and external pressures.
The graph in the lower right shows the top line (total Organizational Culture) remaining stable over the 200 time ticks in the model, while the level of individual culture (the lower three lines) changes over time as some individuals gain culture from their interaction and some lose. Subsequent models show how positive and negative interaction with the model changes the individual and total culture and performance. More on that in subsequent posts. For the purpose of this one, suffice it to say that, without intervention of some kind, Organizational Culture is usually very stable. In medicine it is virtually ossified, maybe even fossilized at Level 3!
Why? Why don’t more spontaneous advancements in Organizational Culture occur? The answer is “complex”—more on that later as well—but look at what happens: With our current emphasis on individual performance for entry into medical school as well as advancement in the profession, especially in academic medicine, a Level 3 culture is the only way to both gain admittance to the profession as well as to advance in it.
Picture yourself as a pre-med student: you face an enormous task of somehow separating yourself from those who are competing for the same spot. You are the “Lone Warrior” who plays in a zero-sum game. You get in if your fellow applicants fall behind. In my experience, it was Organic Chemistry which weeded out the pack. It was through a quirk of luck that I was placed in the class that had been taught by the Great White Shark of our college. But all my other pre-med compatriots had switched to a new professor. I overslept and couldn’t make the switch in time—this was back when you actually had to hand in a punchcard at an office. It turns out the “new guy” was ten times worse, and the Great White was so glad to only have 2 pre-med students that he gave both of us A’s. Go figure….
Then I found myself actually in medical school. I continued in the drive to be the best so I could get into the residency training program I wanted. I had to do better on the Boards than my fellow students. At least in the preclinical years, we lived and died by the “Z-Score” on our tests. It wasn’t so much what we learned, but how we did in comparison to our fellow students. As long as we knew more than they did, we succeeded. Seeing a pattern here? I was a high-flying Level 3 ace!
Then, something happened, and it happened with a thunderclap. It was called "Morning Report” where we all crashed and burned. No matter what we did, it was really never enough. We became, at best, Level 2 trench dogs, sometimes beaten down to Level 1. And this lasted years, at least through internship and early residency. Then, sometime in residency, at least the glimmer of again flying in the clouds of Level 3 was resurrected. Hey, I can get out of the mud! And how to do this? Well, we could fall back on what we learned and experienced in the old Level 3 days. “We’re great….and by the way, you (or he or she) are/is not.”
So…where does “the strange combination of arrogance and ignorance” come from? It came from an infection that was reinforced over many years. It was like getting chicken pox as a kid, but carrying the virus for life, only for it to flare up again as shingles when under stress.
But is there a miraculous agent that can cure the existing infection and prevent a relapse? I think so. It may even function as a true vaccine to prevent infection in the first place! It is a counter meme that can take those very few in medicine out of the Level 3 they thought was the highest peak and on to something even greater. Some very few times it happens by accident. But Dave Logan wanted to improve on chance and developed tools to make the journey a bit more likely. That comes next.
One sobering thought: Organizational Culture and the resulting increase in Organizational Performance can both be a good, and a bad thing. Organized Crime has a high level of Organizational Performance! It indeed has a “pattern of, and capacity for, adaptation based on a shared history, core values, purpose and future”. It may even be seen through a “diversity of perspective”. But the core values and purpose make all the difference in the product. Organizational Culture should be viewed as a transformation function that takes a substrate, such as Organizational Knowledge or Effort and translates it into an output. The efficiency of that transfer is dependent upon the level of the culture.
Great read, especially on a day where our national appointed, not elected, leaders suggest God giving us 2 arms is for solely the COVID shot and the FLU shot. Maybe a better use of 2 arms is to write thought-provoking pieces instead of a 5th booster




Great read, especially on a day where our national appointed, not elected, leaders suggest God giving us 2 arms is for solely the COVID shot and the FLU shot. Maybe a better use of 2 arms is to write thought-provoking pieces instead of a 5th booster
Love this Russ. We’re still working on leveling up Medicine Forward to a stage 4 culture. Great reminder of why it matters!